
Two Industrial Radiography Accidents
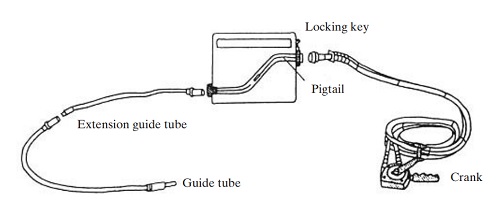
Industrial radiography is a widely used form of non-destructive testing, used to examine welds, pipes, structural steel, and other objects for defects. Radiography can be performed on new welds or new components prior to use, as well as being performed as a regular preventative maintenance inspection. The process is similar to taking an x-ray, using a gamma-emitting source in lieu of an x-ray tube; the nuclide and activity used depend on the material being examined and its thickness. A typical setup consists of a radiography “camera” made of lead or depleted uranium that shields the source when it’s not in use. Connected to one side of the camera is a guide tube running from the camera to the location where the source will be placed (against a new weld, for example); a second tube with a cable and crank is connected to the other side of the camera. This cable connects to the source and the crank is used to extend the cable and source into the guide tube, and to retract it again when the “shot” is completed.
While industrial radiography is a common technique and is usually conducted without incident, it occasionally goes wrong; lost sources have injured or killed people in many countries over the years. A frequent point of failure is the “pigtail” connecting the source to the drive cable. The two incidents related here both originated with the failure of this pigtail, although the incidents progressed differently after this failure.
Accident 1 – Cochabamba, Bolivia
What happened:
In April, 2002 an industrial radiographer was obtaining images in Cochabamba, Bolivia – a city about 400 km (240 miles) from the capital of La Paz. The radiographer had been performing industrial radiography and, at the end of the work, he went to secure the source for shipment. He withdrew the source into the camera and went to seal the camera but could not do so. Assuming that the source had been retracted into the camera and that dirt or grit was interfering with the mechanism he finally rolled up the guide tube, put it into a box, and put the device and box into the cargo compartment of a bus to La Paz. The radiographer reported that he never considered the possibility that the source might not have been fully retracted into the shield, however he never confirmed his assumption by performing a radiation survey, which would have immediately revealed the problem.
Upon arrival the camera and guide tube were retrieved by some of the company’s staff, who put them into a taxi for the trip to the company’s offices. When they arrived they discovered that the radioactive source had not been retracted into the camera but was, instead, stuck in the guide tube and had been irradiating the radiographer, his assistant, the passengers on the bus, the company’s personnel who picked up the package, and their taxi driver. The workers performed a radiation survey and realized that the source was not retracted into the camera because the source had become unattached from the drive cable; they were able to reattach the source and retracted it into the camera within 30-45 minutes.
Nuclide(s) and activity:
The source was about 18 Ci (0.67 TBq) of Ir-192.
Response:
The Bolivian government was notified by telephone on April 15 and by letter two days later. Based on the information initially provided the government estimated the radiographer and others involved in the radiography and source recovery might have received a dose as high as 72 rem and they recommended medical examination of each of them; as more information became available the regulatory agency realized that passengers on the bus, the bus driver, and taxi driver were also exposed to radiation. Further dose calculations showed that passengers might have been exposed toa s much as 250 rem, although later medical testing (chromosomal aberration analysis) showed that nobody received even half that much radiation. Later dose reconstruction measurements and calculations indicated that the most-exposed individual (the radiographer) was likely to have received 18.5 rem with a maximum dose of no more than 50 rem – substantially lower than initial calculations.
The regulatory authorities penalized the radiography firm by fining them, suspending them from work, and seizing and decommissioning their radiography source and returning it to the manufacturer.
Health effects:
Although the initial dose estimates, based on estimates of the amount of time spent performing various tasks, indicated doses greatly in excess of what is required to cause radiation sickness, no workers nor passengers developed radiation sickness or experienced any changes in blood cell counts; the three most-exposed workers showed minor elevations in chromosomal damage but showed no other biological indications of radiation exposure.
Contributing factors:
While investigating this accident the IAEA noted several factors that contributed to this accident; these included several factors that were within the control of the company:
- The company had a poor safety culture, including out-of-date procedures that were not consistently enforced.
- The radiographers had not received adequate radiation safety training.
- The company lacked an effective preventative maintenance program.
- The radiographer was not wearing an individual alarming radiation monitor.
- Transportation of the source violated many regulatory requirements.
Conclusions:
Industrial radiography sources can be dangerously radioactive and they have caused a number of deaths around the world. That this incident did not lead to any injuries or fatalities was due in large part to the relatively low activity of the source (it is not uncommon for radiography sources to contain up to 100 curies of activity) – the company got lucky.
Had any one of the contributing factors noted above been addressed satisfactorily this accident would not have occurred. Had the radiographer received adequate radiation safety training, had the company trained on and enforced its safety policies, had the radiographer performed a radiation survey (as required by regulations) or worn an alarming personal dosimeter – any of these would have led the radiographer to recognize that the source was not retracted into the camera.
Accident 2- Gilan, Iran
What happened:
In July, 1996 a worker at a fossil fuel power plant in Gilan, Iran noticed a shiny metal pencil-shaped object lying in a trench; curious, he put it in his shirt pocket and went on with his work. An hour and a half later the worker began feeling nauseous, dizzy, and had a burning feeling in his chest; he connected these symptoms with the item he’d picked up and he returned it to the trench where he’d found it. The radiography team had realized the source was missing and began a search; they located it about a half hour after it was returned to the trench, returned it to the shield, and informed the site manager. While they had performed radiation surveys following retraction of the source into the shield, the source had fallen into a trench which shielded the radiation and the loss of the source was not recognized.
A few hours later the worker told some colleagues about finding the metal object and that he was feeling ill; they told him to tell the site manager, who realized that the worker’s symptoms were likely due to exposure to radiation from the source. The manager reported the incident to Iran’s radiological regulatory authority, who began an investigation and medical response.
Nuclide and activity:
Ir-192, 5 Ci
Response:
The Atomic Energy Organization of Iran tested 600 workers, sending 55 of them to their headquarters in Tehran for medical and hematological examination. The AEOI provided long-term follow-up medical care for the worker; no other employees were affected by radiation exposure.
Health effects:
The worker suffered a number of medical problems that unfolded over the course of several years. These included skin burns on the chest, the hand used to pick up the source, and the thigh. Additional effects included postural changes due to a skin graft on the chest, thickened skin on the left palm, and contraction of some of the muscles and ligaments of the right elbow.

Lessons learned:
While the site handled this incident relatively well (with the exception of not realizing the source had become unattached earlier), there were some medical lessons learned during this incident that were related to treating radiation injury and are not likely to be useful to anyone other than physicians. However, there are some radiation safety-related observations that are relevant:
- All personnel, including laborers and other unskilled workers, should be aware that radiography is occurring.
- All personnel should know what radiography sources look like and how to respond if one is found.
- Personnel involved in radiography should be aware of the potential for a source to fall into a shielded location and should perform post-shot radiation surveys accordingly.
Conclusions:
A 5-Ci Ir-192 source produces a radiation dose rate of “only” about 2 R/hr at a distance of 1 m; this dose rate is not normally considered to be dangerously high. While this exposure did not lead to the worker’s death, it did cause serious radiation injury, showing that even a source of this activity can be dangerous at a close distance. Only the worker’s linking his symptoms to the odd metal object he’d picked up and the site manager’s astutely connecting this to the radiographer’s report resulted in the prompt recognition of this incident.